Assessing Workplace Health and Safety Strategies, Trends, and Barriers through a Statewide Worksite Survey


Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Survey Responses
3.2. Workplace Health Governance and Planning Strategies
3.3. Workplace Health Governance and Planning Strategies: Multivariable Analysis
3.4. Workplace Safety Policies
3.5. Workplace Safety Policies: Multivariable Analysis
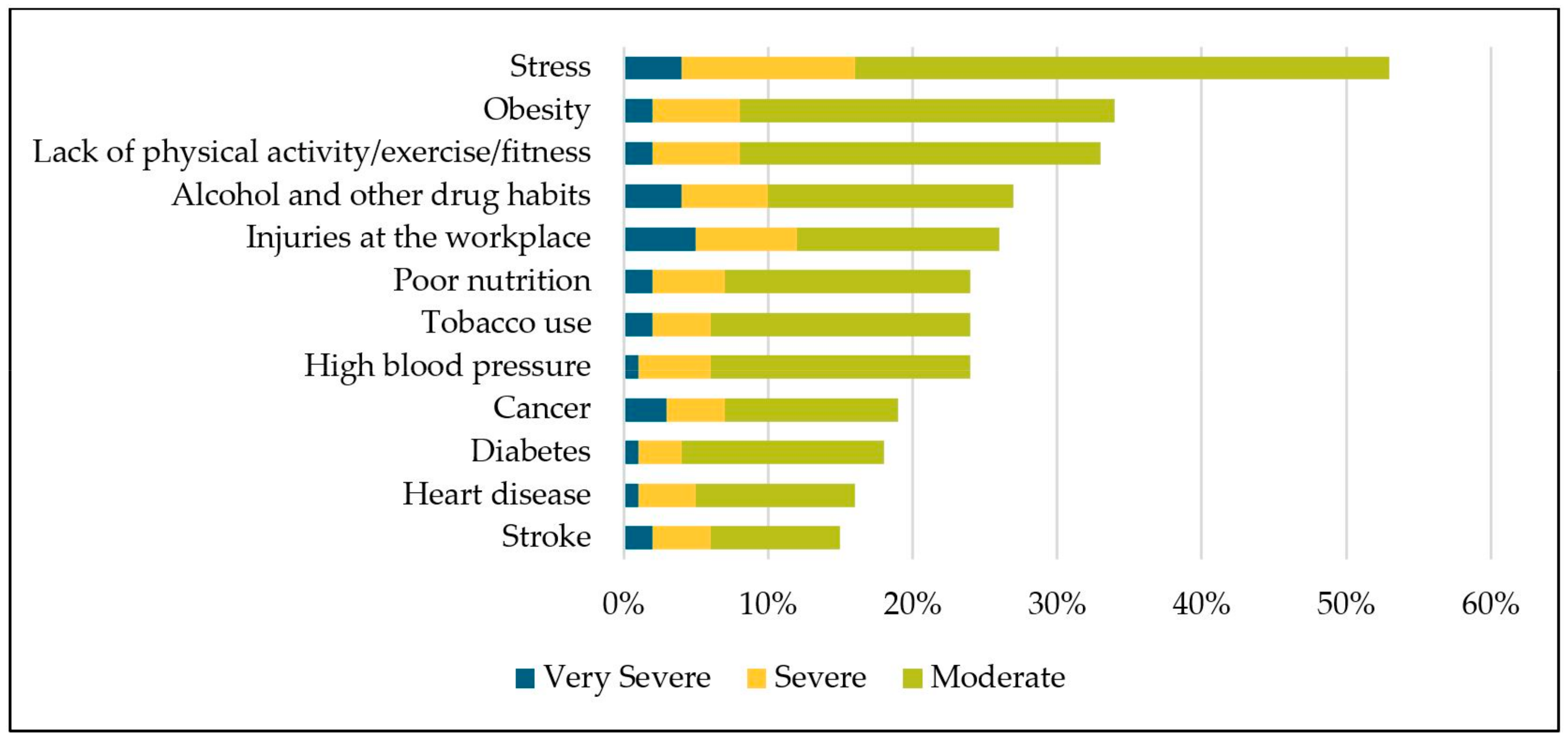
3.6. Negative Impacts of Employee Health Issues
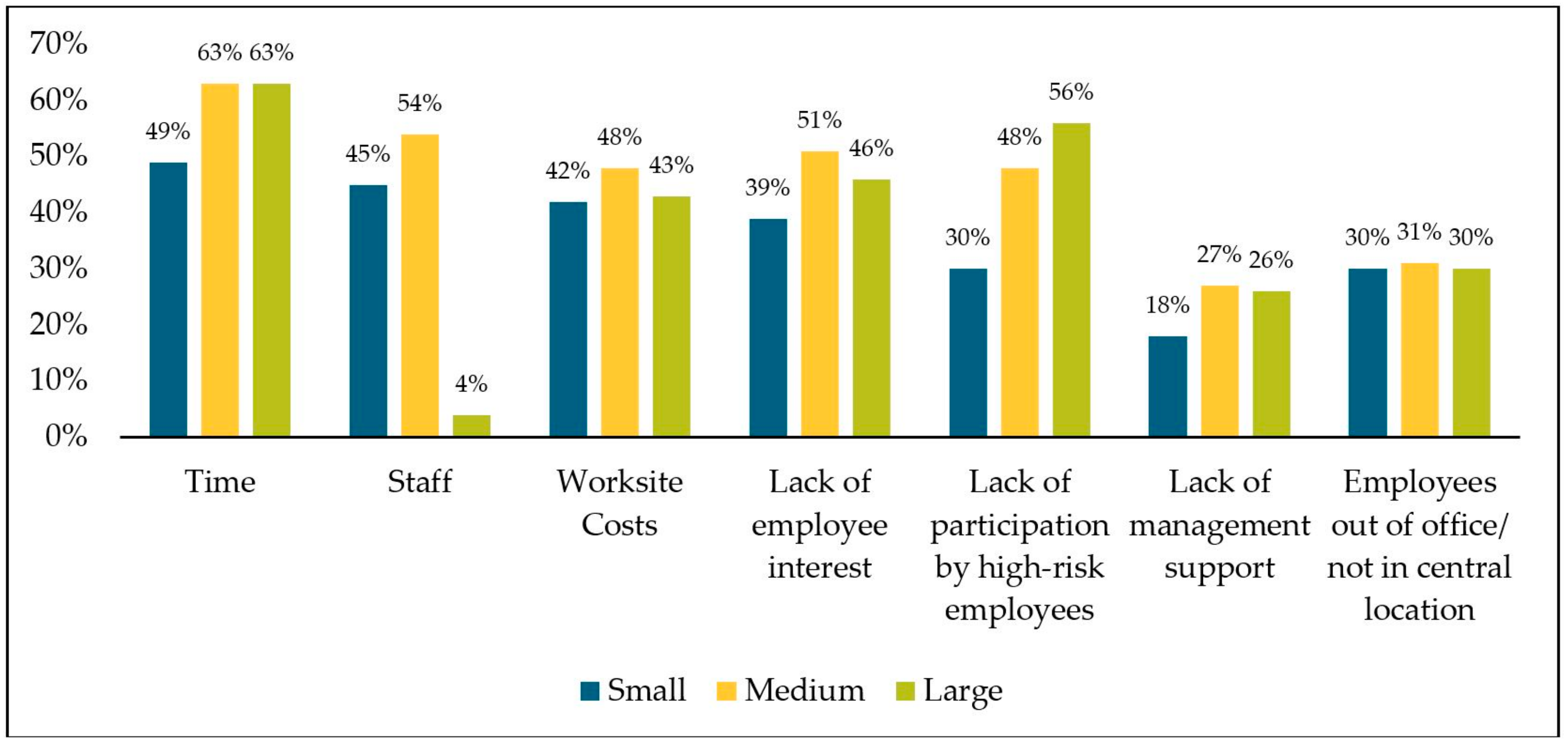
3.7. Barriers in Implementing Workplace Health and Wellness Strategies
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kochanek, K.D.; Murphy, S.L.; Xu, J. Deaths: Final data for 2011. Natl. Vital Stat. Rep. 2015, 63, 1–120. [Google Scholar] [PubMed]
- Gerteis, J.; Izrael, D.; LeRoy, L.; Deitz, D.; Ricciardi, R.; Miller, T.; Basu, J. Multiple Chronic Conditions Chartbook; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2014. [Google Scholar]
- National Center for Chronic Disease Prevention and Health Promotion. The Power of Prevention: Chronic Disease… the Public Health Challenge of the 21st Century 2009. Available online: https://www.cdc.gov/chronicdisease/pdf/2009-Power-of-Prevention.pdf (accessed on 19 January 2019).
- U.S. Bureau of Labor Statistics. Current Population Survey: Labor Force Statistics. Available online: https://data.bls.gov/timeseries/LNS12000000 (accessed on 4 April 2019).
- Aldana, S.G. Financial impact of health promotion programs: A comprehensive review of the literature. Am. J. Health Promot. AJHP 2001, 15, 296–320. [Google Scholar] [CrossRef] [PubMed]
- Soler, R.E.; Leeks, K.D.; Razi, S.; Hopkins, D.P.; Griffith, M.; Aten, A.; Chattopadhyay, S.K.; Smith, S.C.; Habarta, N.; Goetzel, R.Z.; et al. A systematic review of selected interventions for worksite health promotion. The assessment of health risks with feedback. Am. J. Prev. Med. 2010, 38, S237–S262. [Google Scholar] [CrossRef] [PubMed]
- Baicker, K.; Cutler, D.; Song, Z. Workplace wellness programs can generate savings. Health Aff. Proj. Hope 2010, 29, 304–311. [Google Scholar] [CrossRef] [PubMed]
- Goetzel, R.Z.; Ozminkowski, R.J. The health and cost benefits of work site health-promotion programs. Annu. Rev. Public Health 2008, 29, 303–323. [Google Scholar] [CrossRef] [PubMed]
- Pelletier, K.R. A review and analysis of the clinical and cost-effectiveness studies of comprehensive health promotion and disease management programs at the worksite: update VIII 2008 to 2010. J. Occup. Environ. Med. 2011, 53, 1310–1331. [Google Scholar] [CrossRef] [PubMed]
- Ortman, J.; Velkoff, V.; Hogan, H. An Aging Nation: The Older Population in the United States; Current Population Reports; U.S. Census Bureau: Washington, DC, USA, 2014; p. 28.
- Anderko, L.; Roffenbender, J.S.; Goetzel, R.Z.; Howard, J.; Millard, F.; Wildenhaus, K.; Desantis, C.; Novelli, W. Promoting prevention through the affordable care act: Workplace wellness. Prev. Chronic. Dis. 2012, 9, E175. [Google Scholar] [CrossRef] [PubMed]
- Goetzel, R.Z.; Pei, X.; Tabrizi, M.J.; Henke, R.M.; Kowlessar, N.; Nelson, C.F.; Metz, R.D. Ten modifiable health risk factors are linked to more than one-fifth of employer-employee health care spending. Health Aff. Proj. Hope 2012, 31, 2474–2484. [Google Scholar] [CrossRef]
- Koh, H.K.; Sebelius, K.G. Promoting prevention through the Affordable Care Act. N. Engl. J. Med. 2010, 363, 1296–1299. [Google Scholar] [CrossRef]
- McCoy, K.; Stinson, K.; Scott, K.; Tenney, L.; Newman, L.S. Health promotion in small business: A systematic review of factors influencing adoption and effectiveness of worksite wellness programs. J. Occup. Environ. Med. 2014, 56, 579–587. [Google Scholar] [CrossRef]
- Mattke, S.; Liu, H.H.; Caloyeras, J.P.; Huang, C.Y.; Van Busum, K.R.; Khodyakov, D.; Shier, V. Workplace Wellness Programs Study: Final Report; RAND Corporation: Santa Monica, CA, USA, 2013. [Google Scholar]
- Goetzel, R.Z.; Henke, R.M.; Tabrizi, M.; Pelletier, K.R.; Loeppke, R.; Ballard, D.W.; Grossmeier, J.; Anderson, D.R.; Yach, D.; Kelly, R.K.; et al. Do workplace health promotion (wellness) programs work? J. Occup. Environ. Med. 2014, 56, 927–934. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Workplace Health Promotion: Planning/Workplace Governance. Available online: https://www.cdc.gov/workplacehealthpromotion/planning/index.html (accessed on 30 January 2019).
- McLellan, D.L.; Cabán-Martinez, A.J.; Nelson, C.C.; Pronk, N.P.; Katz, J.N.; Allen, J.D.; Davis, K.L.; Wagner, G.R.; Sorensen, G. Organizational characteristics influence implementation of worksite health protection and promotion programs: Evidence from smaller businesses. J. Occup. Environ. Med. Am. Coll. Occup. Environ. Med. 2015, 57, 1009–1016. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. CDC Worksite Health ScoreCard Manual: An Assessment Tool to Promote Employee Health and Well-Being; U.S. Department of Health and Human Services: Atlanta, GA, USA, 2019.
- Tamers, S.L.; Chosewood, L.C.; Childress, A.; Hudson, H.; Nigam, J.; Chang, C.-C. Total worker health 2014–2018: The novel approach to worker safety, health, and well-being evolves. Int. J. Environ. Res. Public. Health 2019, 16, E321. [Google Scholar] [CrossRef] [PubMed]
- NIOSH. Fundamentals of Total Worker Health Approaches: Essential Elements for Advancing Worker Safety, Health, and Well-Being; U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health: Cincinnati, OH, USA, 2016.
- Kish, L. Weighting for unequal pi. J. Off. Stat. 1992, 183–200. [Google Scholar]
- Pronk, N. Best practice design principles of worksite health and wellness programs. ACSMs Health Fit. J. 2014, 18, 42–46. [Google Scholar] [CrossRef]
- Payne, J.; Cluff, L.; Lang, J.; Matson-Koffman, D.; Morgan-Lopez, A. Elements of a workplace culture of health, perceived organizational support for health, and lifestyle risk. Am. J. Health Promot. AJHP 2018, 32, 1555–1567. [Google Scholar] [CrossRef]
- Linnan, L.; Bowling, M.; Childress, J.; Lindsay, G.; Blakey, C.; Pronk, S.; Wieker, S.; Royall, P. Results of the 2004 national worksite health promotion survey. Am. J. Public Health 2008, 98, 1503–1509. [Google Scholar] [CrossRef]
- Cooklin, A.; Joss, N.; Husser, E.; Oldenburg, B. Integrated approaches to occupational health and safety: A systematic review. Am. J. Health Promot. AJHP 2017, 31, 401–412. [Google Scholar] [CrossRef]
- Haberkorn, J. Health policy brief: The prevention and public health fund. Health Aff. (Millwood) 2012. [Google Scholar] [CrossRef]
- Chait, N.; Glied, S. Promoting prevention under the affordable care act. Annu. Rev. Public Health 2018, 39, 507–524. [Google Scholar] [CrossRef]
- Hannon, P.A.; Garson, G.; Harris, J.R.; Hammerback, K.; Sopher, C.J.; Clegg-Thorp, C. Workplace health promotion implementation, readiness, and capacity among mid-sized employers in low-wage industries: A national survey. J. Occup. Environ. Med. Am. Coll. Occup. Environ. Med. 2012, 54, 1337–1343. [Google Scholar] [CrossRef] [PubMed]
- Glasgow, R.E.; McCaul, K.D.; Fisher, K.J. Participation in worksite health promotion: A critique of the literature and recommendations for future practice. Health Educ. Q. 1993, 20, 391–408. [Google Scholar] [CrossRef] [PubMed]
- Stiehl, E.; Shivaprakash, N.; Thatcher, E.; Ornelas, I.J.; Kneipp, S.; Baron, S.L.; Muramatsu, N. Worksite health promotion for low-wage workers: A scoping literature review. Am. J. Health Promot. AJHP 2018, 32, 359–373. [Google Scholar] [CrossRef] [PubMed]
- Merchant, J.A.; Lind, D.P.; Kelly, K.M.; Hall, J.L. An employee total health management-based survey of Iowa employers. J. Occup. Environ. Med. Am. Coll. Occup. Environ. Med. 2013, 55, S73–S77. [Google Scholar] [CrossRef] [PubMed]
- Gomaa, A.E.; Tapp, L.C.; Luckhaupt, S.E.; Vanoli, K.; Sarmiento, R.F.; Raudabaugh, W.M.; Nowlin, S.; Sprigg, S.M. Occupational traumatic injuries among workers in health care facilities—United States, 2012–2014. MMWR Morb. Mortal. Wkly. Rep. 2015, 64, 405–410. [Google Scholar] [PubMed]
- Helmkamp, J.C.; Lincoln, J.E.; Sestito, J.; Wood, E.; Birdsey, J.; Kiefer, M. Risk factors, health behaviors, and injury among adults employed in the transportation, warehousing, and utilities Super SECTOR. Am. J. Ind. Med. 2013, 56, 556–568. [Google Scholar] [CrossRef]
- Sieber, W.K.; Robinson, C.F.; Birdsey, J.; Chen, G.X.; Hitchcock, E.M.; Lincoln, J.E.; Nakata, A.; Sweeney, M.H. Obesity and other risk factors: The national survey of U.S. long-haul truck driver health and injury. Am. J. Ind. Med. 2014, 57, 615–626. [Google Scholar] [CrossRef]
- Marcum, J.L.; Chin, B.; Anderson, N.J.; Bonauto, D.K. Self-reported work-related injury or illness—Washington, 2011–2014. MMWR Morb. Mortal. Wkly. Rep. 2017, 66, 302–306. [Google Scholar] [CrossRef]
- Luckhaupt, S.E.; Calvert, G.M. Prevalence of coronary heart disease or stroke among workers aged <55 Years—United States, 2008–2012. MMWR Morb. Mortal. Wkly. Rep. 2014, 63, 645–649. [Google Scholar]
- Dong, X.S.; Wang, X.; Largay, J.A. Occupational and non-occupational factors associated with work-related injuries among construction workers in the USA. Int. J. Occup. Environ. Health 2015, 21, 142–150. [Google Scholar] [CrossRef] [Green Version]
- U.S. Bureau of Labor Statistics. 2017 Survey of Occupational Injuries & Illnesses Charts Package. Available online: https://www.bls.gov/iif/osch0062.pdf (accessed on 30 January 2019).
- Apostolopoulos, Y.; Sönmez, S.; Mona, S.; Haldeman, L.; Strack, R.; Jones, V. Barriers to truck drivers’ healthy eating: Environmental influences and health promotion strategies. J. Workplace Behav. Health 2011, 26, 122–143. [Google Scholar] [CrossRef]
- Lemke, M.; Apostolopoulos, Y. Health and wellness programs for commercial motor-vehicle drivers: Organizational assessment and new research directions. Workplace Health Saf. 2015, 63, 71–80. [Google Scholar] [CrossRef]
- Anderson, N.J.; Smith, C.K.; Byrd, J.L. Work-related injury factors and safety climate perception in truck drivers. Am. J. Ind. Med. 2017, 60, 711–723. [Google Scholar] [CrossRef]
- Pronk, N.P. Integrated worker health protection and promotion programs: Overview and perspectives on health and economic outcomes. J. Occup. Environ. Med. Am. Coll. Occup. Environ. Med. 2013, 55, S30–S37. [Google Scholar] [CrossRef]
- Sorensen, G.; McLellan, D.; Dennerlein, J.T.; Pronk, N.P.; Allen, J.D.; Boden, L.I.; Okechukwu, C.A.; Hashimoto, D.; Stoddard, A.; Wagner, G.R. Integration of health protection and health promotion: Rationale, indicators, and metrics. J. Occup. Environ. Med. Am. Coll. Occup. Environ. Med. 2013, 55, S12–S18. [Google Scholar] [CrossRef]
- Loeppke, R.R.; Schill, A.L.; Chosewood, L.C.; Grosch, J.W.; Allweiss, P.; Burton, W.N.; Barnes-Farrell, J.L.; Goetzel, R.Z.; Heinen, L.; Hudson, T.W.; et al. Advancing workplace health protection and promotion for an aging workforce. J. Occup. Environ. Med. 2013, 55, 500–506. [Google Scholar] [CrossRef]
- Anger, W.K.; Kyler-Yano, J.; Vaughn, K.; Wipfli, B.; Olson, R.; Blanco, M. Total worker health intervention for construction workers alters safety, health, well-being measures. J. Occup. Environ. Med. 2018, 60, 700–709. [Google Scholar] [CrossRef]
- Peters, S.E.; Grant, M.P.; Rodgers, J.; Manjourides, J.; Okechukwu, C.A.; Dennerlein, J.T. A cluster randomized controlled trial of a Total Worker Health® intervention on commercial construction sites. Int. J. Environ. Res. Public. Health 2018, 15, E2354. [Google Scholar] [CrossRef]
- Anger, W.K.; Elliot, D.L.; Bodner, T.; Olson, R.; Rohlman, D.S.; Truxillo, D.M.; Kuehl, K.S.; Hammer, L.B.; Montgomery, D. Effectiveness of total worker health interventions. J. Occup. Health Psychol. 2015, 20, 226–247. [Google Scholar] [CrossRef]
- Carr, L.J.; Leonhard, C.; Tucker, S.; Fethke, N.; Benzo, R.; Gerr, F. Total worker health Intervention increases activity of sedentary workers. Am. J. Prev. Med. 2016, 50, 9–17. [Google Scholar] [CrossRef]
- Bradley, C.J.; Grossman, D.C.; Hubbard, R.A.; Ortega, A.N.; Curry, S.J. Integrated interventions for improving total worker health: A panel report from the National Institutes of Health pathways to prevention workshop: Total worker health—What’s work got to do with it? Ann. Intern. Med. 2016, 165, 279–283. [Google Scholar] [CrossRef]
- Fishta, A.; Backé, E.-M. Psychosocial stress at work and cardiovascular diseases: An overview of systematic reviews. Int. Arch. Occup. Environ. Health 2015, 88, 997–1014. [Google Scholar] [CrossRef]
- Chandola, T.; Brunner, E.; Marmot, M. Chronic stress at work and the metabolic syndrome: Prospective study. BMJ 2006, 332, 521–525. [Google Scholar] [CrossRef]
- Kubo, J.; Goldstein, B.A.; Cantley, L.F.; Tessier-Sherman, B.; Galusha, D.; Slade, M.D.; Chu, I.M.; Cullen, M.R. Contribution of health status and prevalent chronic disease to individual risk for workplace injury in the manufacturing environment. Occup. Environ. Med. 2014, 71, 159–166. [Google Scholar] [CrossRef]
- Thiese, M.S.; Hanowski, R.J.; Kales, S.N.; Porter, R.J.; Moffitt, G.; Hu, N.; Hegmann, K.T. Multiple conditions increase preventable crash risks among truck drivers in a cohort study. J. Occup. Environ. Med. 2017, 59, 205–211. [Google Scholar] [CrossRef]
- Schulte, P.A.; Pandalai, S.; Wulsin, V.; Chun, H. Interaction of occupational and personal risk factors in workforce health and safety. Am. J. Public Health 2012, 102, 434–448. [Google Scholar] [CrossRef]
- Taylor, A.W.; Pilkington, R.; Montgomerie, A.; Feist, H. The role of business size in assessing the uptake of health promoting workplace initiatives in Australia. BMC Public Health 2016, 16, 353. [Google Scholar] [CrossRef]
- Grosch, J.W.; Alterman, T.; Petersen, M.R.; Murphy, L.R. Worksite health promotion programs in the U.S.: Factors associated with availability and participation. Am. J. Health Promot. AJHP 1998, 13, 36–45. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| 2010 (n = 1512) | 2013 (n = 1352) | 2016 (n = 1920) | ||||
|---|---|---|---|---|---|---|
| n | (%) | n | (%) | n | (%) | |
| Worksite Size * | ||||||
| Small (10 to 49 employees) | 574 | (38.0) | 582 | (43.1) | 881 | (45.9) |
| Medium (50 to 199 employees) | 695 | (46.0) | 510 | (37.7) | 839 | (43.7) |
| Large (more than 200 employees) | 243 | (16.1) | 260 | (19.2) | 200 | (10.4) |
| Industry Sector * | ||||||
| Health Care and Social Assistance | 262 | (17.3) | 260 | (19.6) | 342 | (17.8) |
| Wholesale and Retail Trade | 237 | (15.7) | 197 | (14.8) | 269 | (14.0) |
| Information, Finance, and Management Services | 189 | (12.5) | 188 | (14.2) | 236 | (12.3) |
| Other Services | 225 | (14.9) | 185 | (13.9) | 219 | (11.4) |
| Educational Services | 148 | (9.8) | 149 | (11.2) | 183 | (9.5) |
| Construction | 92 | (6.1) | 58 | (4.4) | 180 | (9.4) |
| Manufacturing | 169 | (11.2) | 141 | (10.6) | 171 | (8.9) |
| Public Administration | 113 | (7.5) | 80 | (6.0) | 130 | (6.8) |
| Transportation and Warehousing | 42 | (2.8) | 37 | (2.8) | 143 | (7.5) |
| All Other Sectors | 35 | (2.3) | 34 | (2.6) | 47 | (2.5) |
| Health Promotion Committee *,‡ | Coordinator Responsible for Employee Health Promotion *,†,‡ | Staff Responsible for Employee Health Promotion *,†,‡ | Funding for Health Promotion in Budget *,† | Written Objectives for Employee Health *,‡ | Stated Mission or Goal Regarding Employee Health *,‡ | |
|---|---|---|---|---|---|---|
| % (CI) | % (CI) | % (CI) | % (CI) | % (CI) | % (CI) | |
| Industry Sector | ||||||
| Wholesale and Retail Trade | 12.6 (9.8–15.4) | 15.2 (12.1–18.3) | 10.9 (8.3–13.5) | 10.5 (7.9–13.1) | 10.6 (7.9–13.2) | 10.3 (7.7–12.9) |
| All Other Sectors | 29.9 (19.8–39.9) | 27.4 (17.8–37.1) | 22.6 (13.6–31.7) | 27.4 (17.8–37.0) | 15.1 (8.2–21.9) | 11.0 (5.1–16.9) |
| Construction | 6.2 (3.3–9.0) | 4.4 (2.3–6.6) | 2.6 (1.0–4.2) | 5.2 (2.4–8.1) | 5.0 (2.3–7.7) | 2.9 (0.6–5.1) |
| Educational Services | 64.3 (58.1–70.4) | 57.8 (51.5–64.0) | 47.5 (41.3–53.8) | 19.6 (14.7–24.5) | 22.8 (17.8–27.9) | 24.0 (18.7–29.3) |
| Health Care and Social Assistance | 16.9 (13.9–20.0) | 16.8 (13.7–19.9) | 16.3 (13.2–19.3) | 12.9 (10.2–15.6) | 11.1 (8.6–13.7) | 11.2 (8.7–13.8) |
| Information, Finance, and Management Services | 24 (20.0–28.0) | 25.2 (21.1–29.3) | 18.5 (15.0–22.1) | 21.6 (17.8–25.4) | 13.4 (10.4–16.4) | 13.1 (10.2–16.0) |
| Manufacturing | 21.6 (17.1–26.2) | 23.8 (19.1–28.6) | 20.7 (16.1–25.4) | 19.8 (15.5–24.0) | 15 (11.1–19.0) | 12.3 (8.8–15.7) |
| Other Services | 7.7 (5.4–10.1) | 7.9 (5.5–10.2) | 7.4 (5.0–9.7) | 5.2 (3.3–7.2) | 4.8 (3.0–6.6) | 5.4 (3.4–7.4) |
| Public Administration | 26.0 (19.8–32.3) | 21.1 (15.4–26.9) | 19.5 (13.9–25.2) | 21.1 (15.2–27.0) | 17.1 (11.6–22.7) | 16.4 (11.0–21.9) |
| Transportation and Warehousing | 12.7 (7.7–17.6) | 14.9 (9.7–20.1) | 11.1 (6.3–15.8) | 8.2 (4.4–12.1) | 9.5 (5.5–13.5) | 8.5 (4.6–12.4) |
| Year | ||||||
| 2010 | 16.2 (14.0–18.3) | 15.7 (13.6–17.8) | 12.6 (10.7–14.5) | 11.1 (9.3–12.9) | 10.1 (8.3–11.8) | 9.2 (7.5–10.9) |
| 2013 | 20.0 (17.0–22.6) | 19.7 (17.2–22.2) | 15.7 (13.4–18.0) | 13.3 (11.2–15.4) | 11.9 (9.9–13.9) | 11.3 (9.4–13.2) |
| 2016 | 21.2 (18.9–23.5) | 21.4 (19.2–23.7) | 18.5 (16.4–20.7) | 15.6 (13.6–17.7) | 12.2 (10.5–14.0) | 12.1 (10.3–13.9) |
| Worksite Size | ||||||
| Small | 13.8 (12.2–15.4) | 14.3 (12.7–15.9) | 11.5 (10.0–13.0) | 9.8 (8.4–11.2) | 8.2 (6.9–9.5) | 7.9 (6.6–9.1) |
| Medium | 33.1 (30.6–35.5) | 30.8 (28.4–33.2) | 25.9 (23.7–28.2) | 21.2 (19.2–23.2) | 18.1 (16.2–19.9) | 17.3 (15.4–19.2) |
| Large | 65.1 (60.3–69.8) | 64.0 (59.0–69.0) | 57.2 (52.3–62.0) | 53.5 (48.7–58.3) | 45.8 (41.1–50.4) | 43.5 (38.9–48.1) |
| Total | 19.4 (18.1–20.7) | 19.3 (17.9–20.6) | 15.9 (14.7–17.1) | 13.6 (12.4–14.7) | 11.4 (10.4–12.5) | 11.0 (10.4–12.5) |
| Workplace Health Strategy | Industry Sector | 2010 | 2013 | 2016 |
|---|---|---|---|---|
| Estimate (95% CL) | Estimate (95% CL) | Estimate (95% CL) | ||
| Coordinator responsible for employee health promotion/wellness | Wholesale and Retail Trade (Ref) | 1.00 | 1.00 | 1.00 |
| All Other Sectors | 3.01 (1.29–7.03) | 3.33 (1.38–8.07) | 1.70 (0.92–3.14) | |
| Construction | 0.09 (0.02–0.38) | 0.60 (0.23–1.56) | 0.27 (0.12–0.61) | |
| Educational Services | 2.87 (1.69–4.88) | 11.16 (6.48–19.25) | 17.44 (9.95–30.56) | |
| Health Care and Social Assistance | 1.07 (0.65–1.76) | 1.08 (0.62–1.88) | 1.12 (0.75–1.66) | |
| Information, Finance, and Management Services | 1.73 (1.08–2.79) | 2.07 (1.23–3.51) | 1.68 (1.14–2.47) | |
| Manufacturing | 1.40 (0.81–2.44) | 2.02 (1.07–3.81) | 1.80 (1.10–2.95) | |
| Other Services | 0.22 (0.11–0.45) | 0.95 (0.54–1.68) | 0.50 (0.30–0.82) | |
| Public Administration | 1.44 (0.80–2.59) | 2.23 (1.10–4.52) | 1.26 (0.73–2.18) | |
| Transportation and Warehousing | 0.22 (0.04–1.28) | 1.31 (0.50–3.44) | 1.43 (0.73–2.82) | |
| Health promotion/wellness committee | Wholesale and Retail Trade (Ref) | 1.00 | 1.00 | 1.00 |
| All Other Sectors | 3.72 (1.58–8.77) | 5.38 (2.27–12.76) | 2.30 (1.25–4.26) | |
| Construction | 0.36 (0.14–0.92) | 0.723 (0.29–1.82) | 0.42 (0.20–0.87) | |
| Educational Services | 8.00 (4.65–13.75) | 13.68 (7.78–24.03) | 23.41 (13.09–41.87) | |
| Health Care and Social Assistance | 1.51 (0.89–2.58) | 1.21 (0.68–2.14) | 1.40 (0.93–2.10) | |
| Information, Finance, and Management Services | 2.00 (1.19–3.38) | 2.17 (1.26–3.73) | 2.17 (1.46–3.25) | |
| Manufacturing | 1.55 (0.84–2.85) | 2.16 (1.13–4.15) | 2.02 (1.21–3.37) | |
| Other Services | 0.37 (0.19–0.75) | 0.94 (0.52–1.71) | 0.60 (0.36–1.00) | |
| Public Administration | 2.57 (1.43–4.61) | 3.77 (1.92–7.38) | 1.89 (1.10–3.25) | |
| Transportation and Warehousing | 0.44 (0.10–2.01) | 1.48 (0.56–3.92) | 1.16 (0.54–2.48) | |
| Staff responsible for employee health promotion/wellness | Wholesale and Retail Trade (Ref) | 1.00 | 1.00 | 1.00 |
| All Other Sectors | 4.14 (1.73–9.87) | 2.82 (1.04–7.65) | 1.93 (0.991–3.757) | |
| Construction | 0.08 (0.01–0.55) | 0.42 (0.12–1.50) | 0.24 (0.09–0.632) | |
| Educational Services | 3.52 (1.96–6.33) | 9.04 (5.06–16.16) | 14.01 (8.25–23.81) | |
| Health Care and Social Assistance | 1.78 (1.03–3.06) | 1.50 (0.82–2.73) | 1.44 (0.94–2.20) | |
| Information, Finance, and Management Services | 1.87 (1.07–3.25) | 1.52 (0.82–2.83) | 1.86 (1.22–2.85) | |
| Manufacturing | 1.62 (0.86–3.04) | 2.88 (1.47–5.64) | 2.09 (1.23–3.54) | |
| Other Services | 0.22 (0.09–0.54) | 1.13 (0.60–2.13) | 0.78 (0.48–1.30) | |
| Public Administration | 2.16 (1.14–4.09) | 2.79 (1.32–5.89) | 1.61 (0.90–2.87) | |
| Transportation and Warehousing | 0.15 (0.01–2.07) | 1.70 (0.62–4.71) | 1.25 (0.57–2.73) | |
| Funding for health promotion/wellness in budget | Wholesale and Retail Trade (Ref) | 1.00 | 1.00 | 1.00 |
| All Other Sectors | 6.03 (2.51–14.52) | 6.56 (2.66–16.16) | 2.18 (1.12–4.25) | |
| Construction | 0.36 (0.13–1.02) | 1.20 (0.51–2.86) | 0.26 (0.10–0.67) | |
| Educational Services | 0.94 (0.41–2.12) | 2.36 (1.24–4.49) | 3.36 (1.97–5.71) | |
| Health Care and Social Assistance | 1.56 (0.87–2.79) | 0.91 (0.48–1.73) | 1.19 (0.76–1.85) | |
| Information, Finance, and Management Services | 2.76 (1.59–4.80) | 1.92 (1.07–3.47) | 2.31 (1.51–3.54) | |
| Manufacturing | 1.86 (0.98–3.53) | 3.13 (1.63–6.02) | 1.55 (0.88–2.74) | |
| Other Services | 0.27 (0.12–0.64) | 0.69 (0.35–1.37) | 0.50 (0.28–0.88) | |
| Public Administration | 1.93 (0.98–3.80) | 3.29 (1.60–6.77) | 2.30 (1.32–4.02) | |
| Transportation and Warehousing | 0.05 (<0.001–5.29) | 0.94 (0.29–3.12) | 1.05 (0.46–2.41) | |
| Written objectives for employee wellness/health | Wholesale and Retail Trade (Ref) | 1.00 | 1.00 | 1.00 |
| All Other Sectors | 3.21 (1.28–8.04) | 5.32 (2.11–13.43) | 0.39 (0.12–1.25) | |
| Construction | 0.19 (0.05–0.72) | 1.43 (0.62–3.34) | 0.28 (0.11–0.70) | |
| Educational Services | 1.83 (0.93–3.61) | 3.06 (1.64–5.73) | 3.33 (1.95–5.69) | |
| Health Care and Social Assistance | 1.31 (0.73–2.37) | 0.73 (0.36–1.46) | 1.05 (0.67–1.65) | |
| Information, Finance, and Management Services | 1.47 (0.82–2.63) | 1.27 (0.67–2.42) | 1.17 (0.73–1.86) | |
| Manufacturing | 1.23 (0.62–2.433) | 1.94 (0.94–3.99) | 1.36 (0.76–2.44) | |
| Other Services | 0.24 (0.10–0.58) | 0.93 (0.482–1.80) | 0.34 (0.18–0.65) | |
| Public Administration | 2.17 (1.12–4.19) | 2.13 (0.97–4.69) | 1.52 (0.83–2.77) | |
| Transportation and Warehousing | 0.59 (0.14–2.53) | 0.94 (0.27–3.23) | 1.07 (0.47–2.45) | |
| Stated mission or goal regarding improvement or employee health status | Wholesale and Retail Trade (Ref) | 1.00 | 1.00 | 1.00 |
| All Other Sectors | 1.56 (0.50–4.84) | 3.52 (1.33–9.35) | 0.47 (0.16–1.38) | |
| Construction | 0.17 (0.04–0.70) | 0.97 (0.37–2.50) | 0.08 (0.01–0.40) | |
| Educational Services | 2.35 (1.23–4.46) | 2.95 (1.58–5.51) | 3.32 (1.95–5.68) | |
| Health Care and Social Assistance | 1.37 (0.76–2.48) | 0.96 (0.50–1.83) | 0.98 (0.61–1.56) | |
| Information, Finance, and Management Services | 1.19 (0.64–2.20) | 1.24 (0.65–2.37) | 1.34 (0.84–2.13) | |
| Manufacturing | 0.93 (0.44–1.95) | 1.54 (0.72–3.30) | 1.21 (0.66–2.23) | |
| Other Services | 0.25 (0.10–0.59) | 0.77 (0.39–1.53) | 0.59 (0.34–1.03) | |
| Public Administration | 1.73 (0.87–3.43) | 2.41 (1.12–5.19) | 1.47 (0.80–2.71) | |
| Transportation and Warehousing | 0.32 (0.05–2.15) | 0.88 (0.25–3.08) | 1.13 (0.49–2.61) |
| Require Seatbelts While Driving *,‡ | Require Refrain from Talking on Cell Phone While Driving *,†,‡ | Require Refrain from Texting While Driving *,‡ | Promotes Off-The-Job Safety for Employee and Family *,‡ | Return to Work Program *,‡ | Worksite Safety Committee *,‡ | |
|---|---|---|---|---|---|---|
| % (CI) | % (CI) | % (CI) | % (CI) | % (CI) | % (CI) | |
| Industry Sector | ||||||
| Wholesale and Retail Trade | 67.7 (62.4–73.0) | 54.5 (48.9–60.1) | 60.5 (55.0–66.0) | 28.8 (23.8–33.9) | 59.2 (53.6–64.8) | 62.7 (57.2–68.2) |
| All Other Sectors | 76.0 (64.0–87.9) | 65.1 (51.9–78.4) | 66.7 (79.8–79.8) | 36.5 (23.8–49.2) | 68.1 (55.2–81.0) | 75.5 (63.7–87.3) |
| Construction | 91.6 (88.0–95.2) | 69.9 (63.4–76.4) | 82.2 (77.0–87.3) | 45.3 (38.2–52.3) | 73.1 (66.7–79.5) | 84.6 (79.4–89.8) |
| Educational Services | 71.8 (64.5–79.0) | 63.2 (55.8–70.6) | 66.7 (59.5–73.9) | 42.8 (35.2–50.4) | 46.6 (39.0–54.3) | 83.1 (77.2–89.0) |
| Health Care and Social Assistance | 51.6(46.2–57.1) | 46.2 (40.8–51.6) | 47.6 (42.2–52.9) | 33.2 (28.2–38.2) | 53.6 (48.2–59.1) | 60.6 (55.2–66.1) |
| Information, Finance, and Management Services | 45.1(39.0–51.1) | 36.6 (30.8–42.4) | 41.1 (35.1–47.0) | 19.0 (14.5–23.4) | 42.1 (36.1–48.1) | 48.2 (42.1–54.3) |
| Manufacturing | 74.0 (66.5–81.5) | 61.6 (53.5–69.6) | 64.1 (56.2–72.1) | 41.4 (33.6–49.2) | 72.6 (64.7–80.6) | 90.4 (84.9–95.9) |
| Other Services | 45.2 (39.3–51.1) | 37.5 (31.8–43.2) | 39.6 (33.9–45.3) | 25.8 (20.7–30.9) | 48.3 (42.4–54.1) | 40.7 (35.0–46.4) |
| Public Administration | 73.8 (65.2–82.3) | 48.4 (39.0–57.8) | 50.2 (40.7–59.6) | 33.4 (24.6–42.1) | 55.8 (46.4–65.3) | 74.3 (65.5–83.1) |
| Transportation and Warehousing | 91.5 (86.8–96.3) | 88.0 (82.8–93.3) | 89.4 (84.4–94.4) | 49.8 (40.6–59.0) | 77.8 (70.8–84.7) | 66.7 (57.8–75.6) |
| By Year | ||||||
| 2010 | 56.9 (53.7–60.2) | 41.7 (38.5–44.9) | - | - | - | - |
| 2013 | 61.3 (58.0–64.7) | 50.3 (46.9–53.7) | 54.4 (51.0–57.9) | 30.7 (27.6–33.8) | 55.7 (52.3–59.2) | 63.0 (59.7–66.4) |
| 2016 | 61.9 (58.9–64.9) | 51.2 (48.3–54.2) | 54.7 (51.7–57.7) | 32.5 (29.8–35.2) | 55.2 (52.2–58.2) | 62.1 (59.1–65.1) |
| Worksite Size | ||||||
| Small | 56.9 (54.6–59.2) | 45.0 (42.7–47.2) | 51.8 (49.1–54.5) | 28.5 (26.1–30.9) | 51.1 (48.4–53.9) | 57.2 (54.5–59.9) |
| Medium | 69.8 (67.2–72.4) | 57.1 (54.4–59.9) | 66.2 (63.7–68.8) | 42.5 (39.8–45.3) | 72.7 (70.2–75.1) | 84.6 (82.6–86.5) |
| Large | 78.0 (74.6–81.4) | 62.4 (57.9–66.9) | 68.3 (63.9–72.8) | 61.2 (56.5–65.9) | 80.4 (76.6–84.3) | 89.5 (86.5–92.5) |
| Total | 61.5 (59.3–63.8) | 50.8 48.6–53.1) | 54.6 (52.4–56.9) | 31.8 (29.7–33.8) | 55.5 (53.2–57.8) | 62.5 (60.2–64.7) |
| Workplace Safety Policy | Industry Sector | 2013 | 2016 |
|---|---|---|---|
| Estimate (95% CL) | Estimate (95% CL) | ||
| Require seatbelts while driving | Wholesale and Retail Trade (Ref) | 1.00 | 1.00 |
| All Other Sectors | 1.58 (0.51–4.96) | 1.84 (0.781–4.34) | |
| Construction | 29.49 (2.18–398.55) | 3.07 (1.50–6.24) | |
| Educational Services | 1.08 (0.59–1.98) | 0.88 (0.50–1.56) | |
| Health Care and Social Assistance | 0.36 (0.23–0.58) | 0.42 (0.29–0.61) | |
| Information, Finance, and Management Services | 0.33 (0.20–0.53) | 0.23 (0.16–0.34) | |
| Manufacturing | 1.26 (0.62–2.55) | 1.518 (0.8–2.88) | |
| Other Services | 0.35 (0.22–0.56) | 0.47 (0.31–0.70) | |
| Public Administration | 0.84 (0.41–1.73) | 1.23 (0.67–2.24) | |
| Transportation and Warehousing | 4.98 (1.11–22.43) | 2.71 (1.04–7.03) | |
| Require refrain from talking on cell phone while driving | Wholesale and Retail Trade (Ref) | 1.00 | 1.00 |
| All Other Sectors | 2.20 (0.83–5.79) | 1.632 (0.842–3.162) | |
| Construction | 2.26 (1.14–4.48) | 1.395 (0.888–2.191) | |
| Educational Services | 1.67 (0.97–2.89) | 1.502 (0.892–2.529) | |
| Health Care and Social Assistance | 0.63 (0.41–0.97) | 0.745 (0.531–1.046) | |
| Information, Finance, and Management Services | 0.54 (0.35–0.84) | 0.328 (0.23–0.469) | |
| Manufacturing | 1.12 (0.64–1.97) | 1.36 (0.83–2.23) | |
| Other Services | 0.54 (0.35–0.84) | 0.62 (0.43–0.88) | |
| Public Administration | 0.65 (0.35–1.20) | 0.70 (0.44–1.13) | |
| Transportation and Warehousing | 8.34 (2.22–31.32) | 4.69 (1.95–11.26) | |
| Require refrain from texting while driving | Wholesale and Retail Trade (Ref) | 1.00 | 1.00 |
| All Other Sectors | 2.29 (0.74–7.10) | 1.26 (0.65–2.45) | |
| Construction | 8.07 (2.37–27.46) | 1.91 (1.15–3.18) | |
| Educational Services | 1.11 (0.64–1.94) | 1.46 (0.85–2.52) | |
| Health Care and Social Assistance | 0.39 (0.25–0.60) | 0.65 (0.46–0.92) | |
| Information, Finance, and Management Services | 0.44 (0.28–0.69) | 0.31 (0.22–0.44) | |
| Manufacturing | 0.67 (0.38–1.19) | 1.40 (0.83–2.35) | |
| Other Services | 0.40 (0.25–0.62) | 0.55 (0.38–0.79) | |
| Public Administration | 0.38 (0.20–0.70) | 0.65 (0.40–1.06) | |
| Transportation and Warehousing | 5.76 (1.46–22.70) | 4.58 (1.78–11.77) | |
| Promotes off-the-job safety for employee and family | Wholesale and Retail Trade (Ref) | 1.00 | 1.00 |
| All Other Sectors | 1.89 (0.85–4.24) | 1.39 (0.77–2.53) | |
| Construction | 2.20 (1.22–3.96) | 1.96 (1.28–3.00) | |
| Educational Services | 1.58 (0.97–2.56) | 2.14 (1.34–3.42) | |
| Health Care and Social Assistance | 1.08 (0.712–1.63) | 1.06 (0.76–1.48) | |
| Information, Finance, and Management Services | 0.44 (0.27–0.73) | 0.54 (0.37–0.79) | |
| Manufacturing | 1.72 (1.01–2.92) | 1.62 (1.02–2.55) | |
| Other Services | 0.83 (0.53–1.28) | 1.03 (0.72–1.49) | |
| Public Administration | 0.93 (0.50–1.74) | 1.37 (0.85–2.21) | |
| Transportation and Warehousing | 2.87 (1.39–5.92) | 2.15 (1.20–3.86) | |
| Return to work program | Wholesale and Retail Trade (Ref) | 1.00 | 1.00 |
| All Other Sectors | 2.58 (0.88–7.60) | 4.09 (1.50–11.16) | |
| Construction | 3.24 (1.55–6.78) | 1.23 (0.77–1.98) | |
| Educational Services | 0.65 (0.40–1.06) | 0.61 (0.37–1.01) | |
| Health Care and Social Assistance | 1.07 (0.70–1.61) | 0.53 (0.37–0.74) | |
| Information, Finance, and Management Services | 0.56 (0.37–0.85) | 0.43 (0.30–0.63) | |
| Manufacturing | 3.27 (1.67–6.41) | 1.29 (0.76–2.19) | |
| Other Services | 0.95 (0.63–1.43) | 0.56 (0.39–0.81) | |
| Public Administration | 1.24 (0.66–2.32) | 0.64 (0.39–1.04) | |
| Transportation and Warehousing | 4.46 (1.62–12.30) | 1.68 (0.82–3.46) | |
| Worksite safety committee | Wholesale and Retail Trade (Ref) | 1.00 | 1.00 |
| All Other Sectors | 1.31 (0.54–3.19) | 2.23 (1.04–4.72) | |
| Construction | 2.54 (1.22–5.30) | 2.61 (1.48–4.59) | |
| Educational Services | 3.21 (1.71–6.04) | 2.39 (1.28–4.50) | |
| Health Care and Social Assistance | 0.68 (0.45–1.03) | 0.73 (0.52–1.03) | |
| Information, Finance, and Management Services | 0.60 (0.39–0.92) | 0.38 (0.27–0.55) | |
| Manufacturing | 7.88 (2.9–21.11) | 3.93 (1.93–8.00) | |
| Other Services | 0.36 (0.24–0.53) | 0.36 (0.25–0.51) | |
| Public Administration | 1.86 (0.91–3.78) | 1.29 (0.76–2.18) | |
| Transportation and Warehousing | 1.10 (0.50–2.41) | 1.17 (0.61–2.26) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sedani, A.; Stover, D.; Coyle, B.; Wani, R.J. Assessing Workplace Health and Safety Strategies, Trends, and Barriers through a Statewide Worksite Survey. Int. J. Environ. Res. Public Health 2019, 16, 2475. https://doi.org/10.3390/ijerph16142475
Sedani A, Stover D, Coyle B, Wani RJ. Assessing Workplace Health and Safety Strategies, Trends, and Barriers through a Statewide Worksite Survey. International Journal of Environmental Research and Public Health. 2019; 16(14):2475. https://doi.org/10.3390/ijerph16142475
Chicago/Turabian StyleSedani, Ami, Derry Stover, Brian Coyle, and Rajvi J. Wani. 2019. "Assessing Workplace Health and Safety Strategies, Trends, and Barriers through a Statewide Worksite Survey" International Journal of Environmental Research and Public Health 16, no. 14: 2475. https://doi.org/10.3390/ijerph16142475